
Treatment of autism
The over-riding cause of autism, and developmental delay is functional vitamin B12 deficiency. This deficiency causes lack of energy production in the brain - due to lower production of creatine, lower rates of myelination - due to reduced production of melatonin, lower production of the neurotransmitter acetylcholine - resulting in poor receptive language and expressive language, and lower reasoning "power". The decreased production of melatonin leads to poor gut health and to many of the food intolerances that the children have. In addition, the decreased methylation due to functional B12 deficiency leads to poorer emotional control as several of the neurotransmitter pathways are interrupted.
Vitamin B12 Deficiency and Autism
It is known that overt vitamin B12 deficiency in the neonate can lead to delayed development and poor cognitive development (1-6; Weiss etal, 2004; Shulpis etal, 2004), regression of psychomotor development, brain atrophy and muscular hypotonia (Lucke etal, 2007; Chalouhi etal, 2008). Mechanistically it can be shown that B12 deficiency involves delayed myelination of the nerves (or even demyelination), reduced methylation, with reduced production of the essential energy transfer molecule, creatine, reduced production of acetylcholine, imbalance of neurotrophic and neurotoxic cytokines (Dror and Allen, 2008). It is also known that vitamin B12 loading of the brain occurs via transplacental transfer to the foetus (7,8), so obviously the place to start, if you want to reduce the possibility of having an autistic baby, is to make sure that the mother has sufficient supplies of vitamin B12.
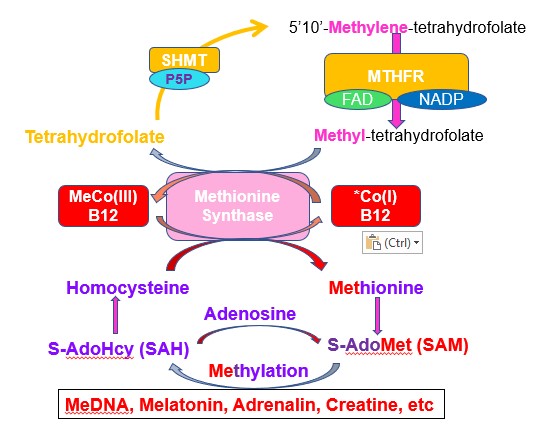
The vitamin B12, though has to be functional, and in all cases of autism that we have data for, there is a functional deficiency in vitamin B12. This functional deficiency has been caused by a deficiency in functional vitamin B2, as the two active forms of vitamin B2, flavin mononucleotide (FMN) and Flavin Adenine Dinucleotide (FAD), together with folate, are essential for maintaining functional vitamin B12 sufficiency, which is essential for methylation and maintainence of S-Adenosylmethionine levels (SAM).. Given the essential role of vitamin B2 in the cycling of vitamin B12, it is important that functional vitamin B2 deficiency be fixed before you can fix the functional B2 deficiency, and before you can displace the inactive vitamin B12 that is in the child.
Vitamin B2 Deficiency and Autism
Central to the cycling of vitamin B12 and the maintenance of it's function is active vitamin B2, as FMN and FAD. Activation of riboflavin (vitamin B2) to FMN and FAD requires Iodine (See section below), Selenium and molybdenum. Many of the mothers of ASD kids and the kids themselves show Iodine, Selenium and/or Molybdenum deficiency. This appears to be one of the reasons why Iodine deficiency in the mothers is the single most preventable cause of developmental delay in the world. From the diagram one can see how critically important Iodine, Selenium and Molybdenum are for the activation of vitamin B6, for the formation of GABA, and for the maintenance of activity of vitamin B12, with the formation of melatonin, for sleep, gut health, myelination, for the formation of iron-sulphur proteins, for energy production, cognition, continence, and many other functions.
The RnBTM protocol for the treatment of Autism
This protocol has been developed to help to overcome functional B2 deficiency in Autism Spectrum Disorder, where it is commonly seen that the functional B2 deficiency is reducing the effectiveness of vitamin B12 supplementation. Lack of methylation due to the functional Methyl B12 deficiency, is the major cause of autism.The protocol overcomes the Paradoxical B12 deficiency often seen in the condition (Paradoxical). The use of the protocol is a preparatory step before injection or transdermal application of vitamin B12.The Vitamin B12 protocol, the RnB Treatment protocolTM is the property of B12 Oils Pty Ltd. The protocol is copyright, as such reproduction in whole or in part constitutes an infringement in the Copyright law. Copyright infringement carries serious penalties, including fines of up to US$150,000 and imprisonment..
Riboflavin and B12 treatment
The assumption is that the vitamin B12 deficiency is caused by lack of functional vitamin B2 (FMN and FAD), which has been caused by a lack of vitamin B2 per se, and a possible lack of Iodine, Selenium and/or Molybdenum, all of which are required for the activation of vitamin B2. Such deficiency may come about due to lack of dietary intake of I/Se/Mo or, as is common, lack of these minerals in the local soils. Riboflavin (vitamin B2) is inactive unless it is first activated within the cell. This activation requires three specific steps, which require Iodine, Selenium and Molybdenum. The protocol revolves around a very gradual introduction of Iodine, Selenium and Molybdenum. Introduction is slow as in extreme deficiency simultaneous administration of all three can have strong side effects. Supplementation with vitamin B2 alone will not work, unless there is sufficient Iodine, Selenium and Molybdenum. The protocol is dependent upon identification of deficiencies in the Hair Metals Test Analysis (HMTA). Thus, the protocol addresses those deficiencies that are identified. It should be noted that everyone requires the recommended daily intake of Iodine, Selenium and Molybdenum every day of their life, hence supplementation must be continued after the protocol has been completed, or the diet must be changed to ensure adequate intake of these essential minerals. Functional B2 deficiency can be established by the Organic Acids Test (OAT)(preferrred) or by TSH/T4/T3 assessment. See OATanalysis This can be used to identify deficiency and to interpret the OAT. For further information on OAT go to OAT
NB - You cannot fix functional B12 deficiency unless you fix functional B2 deficiency! Persons using the protocol need to check by OAT that they have been able to fix the functional B2 deficiency or the B12 deficiency cannot be resolved. It the child is still functionally B2 deficient you cannot make progress in resolving the Developmental Delay! If after following the protocol you do not observe a drop in functional B2 deficiency markers, it is important to identify what the problem is.
NNB The over-riding cause of autism is Functional B12 deficiency, which then results in reduced methylation and low energy efficiency. In turn it is functional B2 deficiency that is causing the functional B12 deficiency, which is what is causing the autism, therefore if you do not fix the deficiencies that cause autism you cannot fix the problem. Implicit in the Protocol, though is the need for biologically active vitamin B12 to be present at all time (See Dopamine Paradox), particularly Methyl B12.
NNNB, most people will have normal to high serum B12 BUT it is inactive. see https://b12oils.com/paradoxical.htm It is necessary to displace the inactive B12 with the mixed Adenosyl/Methyl B12 topical oils. This is an essential part of the protocol. In many instances people cannot make the protocol work until they introduce Methyl or Adenosyl/Methyl B12!! This is due to the Dopamine Paradox, in which thyroid function is inhibited in high dopamine levels (see DopamineParadox). It must be noted, that Neurotypical Delay will/can occur in vitamin B12 deficiency alone, and in this case it is reversed just by addition of vitamin B12.
Iron-sulphur protein production. An essential part of energy production in the cell requires the synthesis of iron-sulphur proteins, this can only occur if sufficient Methyl B12 is present, which is another reason for why you MUST include Adenosyl/Methyl or Methyl B12 as part of the protocol
First start by introducing Iodine
Iodine is at the top of the vitamin B2 activation cascade, as pictured below. (Iodine - I, Selenium - Se, Molybdenum - Mo), For this reason you have to have optimal Iodine levels or the cascade of activation will be compromised.
Iodine build
Start with 50 ug/day for one week and increase to 100 ug/day, week 2. Week 3 and ongoing 150 ug/day. The iodine should be as either the Sodium or Potassium Iodide salt. Iodine does not work, it must be Iodide
Iodide is essential for the production of thyroid hormone (T4)
Natural sources of Iodine are: Seafood, Dairy, Eggs, Grains, and fortified products such as Iodized bread and Iodized salt.
You should avoid goitrogens, such as soy, Cassava, Broccoli, Cauliflower, Cruciferous veggies, and Kale (Goitrogens can affect your iodine levels (iodine-resource.com)_.
Symptoms of over-supplementing with Iodine are generally flu-like symptoms, drowsiness, brain fog following Iodine supplementation, and a drop in TSH below 0.5. RDA for Iodine is 150-300 ug/day (each and every day).
A suitable product is the topically applied Sodium Iodide oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop (~ 74 ug), to 2 drops (150 ug), to 4 drops (300 ug). Topical application avoids interaction of Iodide with food or other supplements
Our data suggests that a suitable target for Iodine can be assessed by monitoring TSH, where a target of between 0.5 and 1.5 should be aimed for. This is in agreement with suggestions made by Kelly (2018) and Cohen and co-workers (2018) and Hanz and co-workers (2020). If your TSH is above 1.5, then you need more Iodine, if it is below 0.5 you may need less Iodine. Avoid using excess Iodide (greater than 600 ug/day). You can assess Iodine sufficiency by urinary output.
Selenium build
After 2 weeks of Iodide supplementation (week 3), continue with the Iodide and add 25 ug/day Selenite and slowly build to 200 ug/day. Start with 25 ug/day for one week and increase to 50 ug/day, week 2. Week 3, 100 ug/day, with week 4 and ongoing 200 ug/day. Adjust doses for children.
Selenite is essential for the conversion of T4 to T3, which is then used to turn on the production of the enzyme Riboflavin kinase which converts riboflavin to FMN.
The RDA for Selenium is 55-200 ug/day, and the aim is to achieve this. In children under 10 aim for 55ug, for adults 200 ug.The selenium should be as the Selenite, or Selenate salt, but should not be Selenomethionine or Selenium chelates, or Selenium amino acids complex, each of which has been shown not to work.
Natural sources of Selenium are: Eggs, Tuna, Shrimp, Beef, Turkey, and wheat from Selenium sufficient soils. Organic foods or gluten-free foods are often low in Selenium as too wheat from selenium depleted soils such as the UK, much of Europe, New Zealand, much of Australia and many States in the USA.
Avoid administering any product with diatomaceous earth, fulvic acid, large dose vitamin C or those with citrate as a preservative, as they can reduce absorption of Selenite (Robinson etal, 1985; Ip, 1986)
Avoid natural source of Calcium, as these bind up the Selenite, thus avoid giving the material in milk. Similarly avoid giving the material in acids, particularly vitamin C and citric acid, as these reduce the Selenite and make it non-available.
A suitable product is the topically applied Sodium Selenite oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop (~ 25 ug), to 8 drops (200 ug). Topical application avoids interaction of Selenite with food or other supplements, which is commonly seen with oral products.
At this stage, T3 should start to turn on the production of riboflavin kinase, which will enable conversion of riboflavin to FMN. This, though is only the first step in riboflavin activation.
Molybdenum build
At week 4, continue with the Iodide and Selenite. Start with 50 ug/day Molybdenum (as the Molybdate salt) and gradually increase to at least 200 ug/day. Some adults have been found to need as much as 300 ug/day. The Molybdenum should be sodium or ammonium Molybdate, NOT a Molybdenum chelate or Molybdenum or Molybdate chelate or Molybdenum amino acids complex. Half the doses for children under 10. The RDA for Molybdenum is 100-300 ug/day. Our studies have shown that over 50% of children with autism are Molybdenum deficient. Similarly studies in 2000 showed that 35% of children were Molybdenum deficient and responded to Molybdenum treatment (Waring and Klovrza 2000)
Molybdenum is also essential for the activity of Sulfite oxidase, which inactivates neurotoxic Sulphite. It is also essential for nitrate reductase, and xanthine oxidase.
Natural sources of Molybdenum are lentils, peas, beans, oats, barley, bread, pasta, but only if they are grown in Molybdenum sufficient soils that are basic.
Avoid natural source of Calcium, as these bind up the Molybdate, thus avoid giving the material in milk. Similarly avoid giving the material in acids, particularly vitamin C and citric acid, as these reduce the Molybdate and make it non-available.
A suitable product is the topically applied Sodium Molybdate oil (https://b12oils.com/order.htm ) which can be really titrated up from one drop (~ 50 ug), to 8 drops (400 ug). Topical application avoids interaction of Molybdate with food or other supplements, which is commonly seen with oral products.
NB, Molybdenum build is essential for the activity of FAD synthase (Giancaspero et al, 2015), which is essential for the conversion of FMN to FAD. FAD is a required co-factor for MTHFR and works with FMN for the activity of MTRR. As such FMN and FAD are required for effective cycling of Methyl B12, and hence for methylation. One could argue, that the Molybdenum build is arguably one of the most important steps in the protocol, and as such is as important as Iodide and Selenite.
Vitamin B2 (riboflavin) build
At week 4 you can slowly start to introduce vitamin B2. Start with 2 mg/day for week 4, 5 mg/day for week 5 and 10 mg/day ongoing (after week 6). You must keep going with the Iodine, Selenium and Molybdenum. It is essential that active riboflavin sufficiency is achieved, or the activation of vitamin B12 will not be complete and active B12 deficiency will still be present. There is currently no B2 (riboflavin oil) so you would need to use an oral formulation.
Low dietary vitamin B2, B12, folate and vitamin D have been shown to affect thyroid function, hence these should be introduced as soon as practicable (Krishnamurthy 2021). In addition, diets high in fats require more B2 for processing and this too affects thyroid function (Sayre and Lechleiter, 2012)
Vitamin B12 (Adenosyl/Methyl B12) build
Studies have shown that it is important to have the active forms of vitamin B12, Adenosyl and Methyl B12 present, to displace inactive serum vitamin B12 - even though levels may be very high. Supplementation should start as soon as is practicable. Start with the mixed Adenosyl/Methyl B12 oil mixture obtainable from B12Oils. It may be necessary to start with just a drop of oil, or use a dropper. Apply the oil into an area of clean dry skin and rub it in like a massage oil. If the child/adult can tolerate the drop, then on the following day increase to 2 drops and gradually increase to a whole squirt/dose. NB you cannot get enough vitamin B12 to restock the brain of a child or an adult from any oral supplement, whether it be lozenge, high dose oral or even nasal delivery. Note, the effect of the combined ISeMo/B2/B12 will take time to become apparent. Myelination is a slow process, and so is repair of damage that occurs in prolonged B12 deficiency. NNB, most people will have normal to high serum B12 BUT it is inactive. see https://b12oils.com/paradoxical.htm NNB, Thyroid function is determined by the amount of B2 and B12, as these appear to affect feed-back on the thyroid (Krishnamurthy etal, 2021). Studies have shown some benefit from injections of methyl B12 alone (Hendren etal, 2016). Numerous studies using high dose oral vitamin B12 on a range of conditions, including ASD, AD, IBD, fatigue and depression have shown this route NOT to be suitable for treatment (Scholten etal, 2018; Robson adn Alvares, 2016).
NB: The liver is the major storage organ for vitamin B12, and so if there is B12, dud or not, it can keep supplying B12 to the body, and hence keep serum B12 levels very high. The body, though is very good at keeping B12, so it binds up B12 with two main proteins, one is transcobalamin, which takes B12 into cells (active or inactive) and the other is haptocorrin, which binds both active and inactive B12. Once these two are saturated, you really don’t know how much B12 you have, as all you have is a very elevated serum B12. The haptocorrin-bound material is returned to the liver for storage and a small fraction is secreted into the stomach via the Salivary glands, but if it is inactive, then when B12 is taken up from the gut via Intrinsic factor, the B12 that is taken up is inactive. It then is “passed” to transcobalamin, but as it is inactive it is useless.
The way to get around this problem is to have lots of free active B12 (methyl and adenosyl), which is where the topical TransdermOilTM is so good. It is unlikely that this gets bound by either HC, or TC in serum because both are saturated. What appears to happen is it is secreted into bile and then it competes with B12 that is in food, or which was bound to HC, and released in the stomach, so it is competing with inactive B12. Hence the higher your inactive B12 was in the past, the longer you have to compete out the inactive. It also means that you have to make sure you have a continuous stream of active B12 around.
NEVER USE CYANOCOBALAMIN
Iron Deficiency and Autism
Iron deficiency is the most prevalent micronutrient deficiency in the world, and is the primary cause of anemia, affecting roughly one-quarter of the world's population. The brain is highly susceptible to iron deficiency during the late foetal and early neonatal time period. Deficiency at this time is associated with altered expression of genes critical for development and function, iron deficiency at this time causes neurocognitive dysfunction, which may continue even after iron stores have become replete. Iron is essential for oxygen transport in the blood (haemoglobin), for oxygen transport within the cell (myoglobin), for the function of the enzyme aconitase, for the function of many of the enzymes in the electron transport chain, and as a co-factor for various enzymes involved in the synthesis of neurotransmitters, amongst other things.
Iron deficiency is present if ferritin levels are below 70 ng/ml and when levels of urinary citrate are above 150.
Processing of iron inside the cell requires functional B2 and functional B12 sufficiency, hence this should be achieved before iron supplementation is successful. At that time heme iron is the iron source of choice. Inorganic iron is relatively ineffective in fixing iron deficiency and in building up iron stores.
Vitamin D Deficiency and Autism
Correction of vitamin D deficiency is dependent upon fixing B2/B12 and iron deficiency, as per the Nexus TheoryTM. Vitamin D activation requires the conversion to 25OH-vitamin D in the liver. This then is dependent upon conversion of 25-OH vitamin D to 1,25 dihydroxy-vitamin D in the brain. In order for this to happen, the child needs to be exposed to sunlight on the eyes. In the Nexus TheoryTM the activation of vitamin B2 and vitamin B12 is required for the action of the enzymes 25-hydroxyvitamin D3 1-alpha-hydroxylase, which contains a heme iron, Adrenodoxin (also called Ferredoxin), which contains an iron-sulphur protein and Adrenodoxin Reductase (also called Ferredoxin reductase), which contains, FAD, the active form of vitamin B2. The cascade of activation is below. The most important thing is that the final step in activation of vitamin D occurs in the brain following stimulation from the eye. Supplementation should be at least 2000 IU/day. Serum vitamin D should be monitored. Be aware that serum vitamin D is generally measured as 25-OH-vitamin D, not as 1,25 diOH vitamin D. Measurement of the function of vitamin D can be obtained from Organic Acids Analysis of urine. Phosphoric acid should be below 2000.
Final step in activation of vitamin D in the brain.
Vitamin B1 Deficiency and Autism
Both vitamin B2 (as FAD) and vitamin B1 (as TPP) are required for the final step in glucose processing. Since glucose is the preferred energy source in the brain, vitamin B1 supplementation may be required. Elevated pyruvate and alpha-ketoglutarate are indicative of functional B1 deficiency, as too elevated glycolic acid. Supplementation should be with Thiamine, NOT Benfotiamine. Benfotiamine is not taken up from the gut via the thiamine transport mechanism, and studies using very high dose Benfotiamine have been less than conclusive.
Folate Deficiency
Early on in the protocol, avoid folate until the B2 and B12 have been optimized. You can introduce folate (either as folic acid, folinic acid or 5MTHF - 400 ug/day). You can and should try to get folate naturally in the diet by eating leafy green veggies. This will also provide the essential mineral magnesium. Folate is an essential part of the methylation cycle, and introduction of folate will amplify the rate of methylation.
Biotin Deficiency
Many people with ASD or CFS believe that the condition is due to an allergy to eggs, and so avoid them. In this case they will more than likely be biotin deficient. Supplement with 150 ug/day - or introduce eggs once the protocol has been established. Biotin deficiency, when severe enough will mask Adenosyl B12 deficiency, and reduce MMA levels.
Gluten-free Products
Most gluten-free products are deficient in Iodine, Selenium and Molybdenum. Further, they are not fortified with either folate or vitamin B1. Additionally they contain high levels of arsenic, lead and mercury (as they are derived from rice flour) which is readily seen by increased values in Hair Metals Test Analysis. Many people who switch to gluten-free products and feel that they gain some benefit have been found to be sensitive to sulphites and nitrites and are Molybdenum deficient, and so not have active sulphitases, or nitritases..
Creatine
Over 40% of methylation is involved in the production of creatine, however, persons on a traditional carnivore diet get around 50% of their creatine from food. Food derived creatine is mainly used in supplementing muscle creatine, weith brain creatine normally being produced in the brain. Supplementation with creatine, has not generally been effective for replenishing brain creatine (Roschel et al, 2021), however, in extreme deficiency prolonged dosing of 3 gm/day for over a month has shown some benefit.
Choline Deficiency
Choline is part of the essential neurotransmitter acetylcholine. Studies have shown reduced levels of choline in the brains of children with autism and adults with dementia. Eggs are one of the best sources of phosphatidylcholine, but many children are placed on restrictive diets, and so no eggs. Choline, when given orally, is converted to betaine in the liver in those that are functionally deficient in Methyl B12. Supplementation with choline, therefore needs a choline source that by-passes the liver. To date the best supplement appears to be alpha-GPC, and Citicoline. More recently some work has been done in preserving what little acetylcholine there is, using ACE inhibitors (Ure eta al, 2023; Karvatg and Kmchi, 2014; Niederfofer and Helmut, 2003; Grossberg, 2017' Oz et al, 2024).
Factors that can affect the protocol
Any stress that the child faces will affect the level of functional vitamin B2 that the child needs, and so will delay or hinder the ability to achieve functional B2 sufficiency. Examples include, vaccination, child-hood illnesses, such as RSV, colds, flu, foot and mouth, and many such diseases that are rampant in child-care institutions, COVID, COVID vaccination, etc. In addition foods such as goitrogens and those containing cyanoglycosides - Cassava, kale, Boy Choi, broccoli, broccolini, cabbage, soy, rutabago, spinach, etc. High levels of bromide affect Iodide uptake into the thyroid. The most obvious affect is the inability to lower TSH levels with the protocol. Low iron affects the function of thyroid peroxidase and so will affect the formation of T4 in the thyroid. It has also been shown that high levels of fluoride in the drinking water, or in ground water can cause conditions such as Fluorosis, in which TSH levels remain very high, despite Iodide supplementation. It is therefore essential to remove these contaminants before resuming the protocol (Kheradpisheh et al, 2018; Kutlucan etal, 2013).
Medications that interfere with the protocol
It has been found that many of the medications, such as SSRIs, including Risperidone, Tricyclic antidepressants, Monamineoxidase inhibitors, Benzodiazepines, etc affect the success of the protocol and block effective restoration of neurotypical development in children and adults. Until the child/adult has been "weaned" off these drugs, the protocol will not be fully effective. It is important, however, to consult your doctor before you make any such changes in treatments. Side effects of these drugs can be found at
Risperidone Risperidone Side Effects: Common, Severe, Long Term - Drugs.com including : agitation, akathisia, anxiety, constipation, dizziness, drowsiness, dystonia, extrapyramidal reaction, nausea, rhinitis, and weight gain. Other side effects include: abdominal pain, sialorrhea, skin rash, tachycardia, and xeroderma (McCrackenet al 2002; de Araújo et al 2016; Citrome 2017; Maher et al 2012; Ceylan et al 2017; Chaves et al 2013).
SSRIs About Selective Serotonin Reuptake Inhibitors (SSRIs) (healthline.com)
Prevention is better than cure
References/ Useful links
Vitamin B12 deficiency and sleep disorders
Altered Neurotransmitter Metabolites in vitamin B12 deficiency
Complex Interaction between iron, B2, B12 and vitamin D Gregory John Russell-Jones. Complex Interaction between Iron, Vitamin B2, Vitamin B12 and Vitamin D During the Activation of Vitamin D. J Med - Clin Res & Rev. 2024; 8(6): 1-5
Role of vitamin B12 in the synthesis of iron-sulphur proteins J. Medical-Clinical Research & Reviews 2024: 8(11):1-6
The Biochemistry of Autism https://www.intechopen.com/online-first/the-biochemistry-of-autism
Altered Serotonin Metabolism in Functional vitamin B12 deficiency .
Ure A, Cox GR, Haslam R, Williams K. Acetylcholinesterase inhibitors for
autistic spectrum disorders. Cochrane Database Syst Rev. 2023 Jun
1;6(6):CD013851. doi: 10.1002/14651858.CD013851.pub2. PMID: 37267443; PMCID:
PMC10233795.
Karvat, G., Kimchi, T. Acetylcholine Elevation Relieves Cognitive Rigidity and
Social Deficiency in a Mouse Model of Autism. Neuropsychopharmacol 39, 831–840
(2014). https://doi.org/10.1038/npp.2013.274
Niederhofer, Helmut. (2003). Acetylcholinesterase-inhibitors in the treatment of
autistic disorders. Expert review of neurotherapeutics. 3. 409-12.
10.1586/14737175.3.4.409.
Kaye AD, Allen KE, Smith Iii VS, Tong VT, Mire VE, Nguyen H, Lee Z, Kouri M,
Jean Baptiste C, Mosieri CN, Kaye AM, Varrassi G, Shekoohi S. Emerging
Treatments and Therapies for Autism Spectrum Disorder: A Narrative Review.
Cureus. 2024 Jul 2;16(7):e63671. doi: 10.7759/cureus.63671. PMID: 39092332;
PMCID: PMC11293483.
Grossberg S. Acetylcholine Neuromodulation in Normal and Abnormal Learning and
Memory: Vigilance Control in Waking, Sleep, Autism, Amnesia and Alzheimer's
Disease. Front Neural Circuits. 2017 Nov 2;11:82. doi: 10.3389/fncir.2017.00082.
PMID: 29163063; PMCID: PMC5673653.
Oz M, Kury LA, Sadek B, Mahgoub MO. The role of nicotinic acetylcholine
receptors in the pathophysiology and pharmacotherapy of autism spectrum
disorder: Focus on α7 nicotinic receptors. Int J Biochem Cell Biol. 2024
Sep;174:106634. doi: 10.1016/j.biocel.2024.106634. Epub 2024 Jul 31. PMID:
39094731.
Copyright © 2017
wipeoutautism.org. All Rights Reserved.
The statements on this site compose a compendium of generally recognized signs
of Autism. They also are formulated from a summary of relevant
scientific publications. In addition they may contain some forward looking
statements of a general nature.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited