
Biochemistry of Autism
The majority of Institutions involved in the treatment of autism seem to have a very poor understanding of what causes the condition and why it persists. The cause of the condition is though readily apparent once one has a better knowledge of the Biochemistry of Autism. It is already known that several nutritional deficiencies are associated with delayed mental development of young children, including Iodine deficiency (one of the single most important preventable cause of brain damage) (1,2,3), iron deficiency (4,5,6), and vitamin B12 deficiency (7,8,9).It is thus highly likely that such a deficiency or deficiencies may be shown to be the cause of the developmental delay(s), that characterize autism, and that these would show up as metabolic abnormalities in the children. In this regard, it is possible to readily obtain urine samples from children with autism and to analyze these samples to determine if the condition is related to, or caused by nutritional deficiency, and how this affects the bioenergetics (energy production by the body) and neuropharmacology of the children. To this end, we have obtained results from urinary samples from around 200 children with ASD and have been able to compare this data to that obtained from metabolically and clinically normal individuals.
Energetics of Autism
Through the study of bioenergetics it is possible to examine which metabolic functions are normal or different in Autism and hence determine whether nutrient depletion is possibly associated with the development and maintenance of the condition. We like to think of this as "looking under the bonnet" of a car and checking to see what is working and where there are problems.

The main energy sources in the body come from carbohydrates (sugars), fats and from protein, with the brain preferring sugar above all other sources. The heart in contrast prefers fat. (This is similar to the engine in the car, which can use petrol, diesel, gas or ethanol for fuel). The use of these substances generally requires preparation and degradation into small "bight sized" pieces that are converted into energy-yielding organic acids. If these organic acids cannot be used for energy production they appear in the urine and so can indicate a potential block in the enzyme systems involved in processing these Organic Acids. (This is similar to seeing black unburnt fuel coming out the exhaust of a car). Basically the greater the amount of each of the products that appears in urine, the greater the loss of energy that the child has, and the more likely that there is a deficiency in the function of the enzyme responsible for processing the products. (Similar to examining the exhaust gases of a car and using these to optimize how the car performs). There are two main commercially available tests that can be used to analyze these products, the Organic Acids Test (OAT) from Great Plains Laboratories, and a similar test from Genova laboratories. Data from these tests has been used to analyze the metabolism of ASD children. The body uses fuels in a similar way to the way a car uses fuel, with the end product of metabolism (or combustion in the car) being carbon dioxide and water (just as in optimal fuel usage in a car). In order to produce energy, the body uses a series of enzymes to change the fuel into energy, just as the car uses a spark plug to "burn" the fuel. These enzymes often have helpers that make the enzymes work faster, generally these "helpers" are called co-factors, and most often they are vitamins or metals. Just as a car will not work without a spark plug, many of the enzymes will not work without their co-factors. By studying the activities of the enzymes involved in "burning" food, one is able to determine if a particular vitamin or metal is present, as a deficiency in function of an enzyme generally means that there will be an increase in the "unburnt" organic acid.
Metabolism of Glucose in Autism
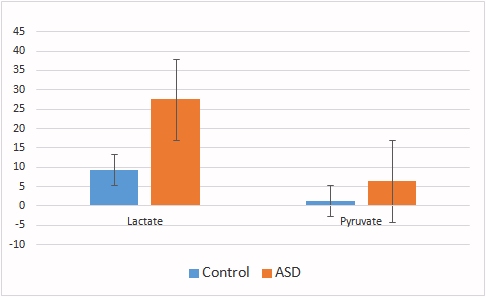
The break-down of glucose (one of the most common sugar molecules in the body), is called glycolysis, and at the end of glycolysis a final product, pyruvate is produced. This product normally is processed by an enzyme called pyruvate dehydrogenase, which converts the pyruvate to acetyl-CoA, an essential intermediate product that can be used by the major energy cycle, the Krebs cycle, or can be converted to fat or used to make the neurotransmitter acetyl-CoA or to make cholesterol, so it is a very important intermediate in the body. If the enzyme, pyruvate dehydrogenase has a problem in its function, pyruvate is not processed and is converted to lactic acid. Examination of the metabolites lactic acid (lactate) and pyruvate, shows that both levels are increased in ASD, suggesting a block in the enzyme pyruvate dehydrogenase. This block has implications for a reduction in the availability of glucose and acetylcholine in the brains of children with ASD. Theoretically from every molecule of glucose that your body uses you can potentially make 38 molecules of the energy unit ATP. If, however, access to the Krebs cycle is restricted or, steps within the cycle are not completed energy can be reduced to as little as 2 units of ATP. A huge loss. The enzyme pyruvate dehydrogenase has three essential co-factors (helpers) for function, TPP (an active form of vitamin B1), FAD (an active form of vitamin B2), and lipoic acid (also known as ALA).
 |
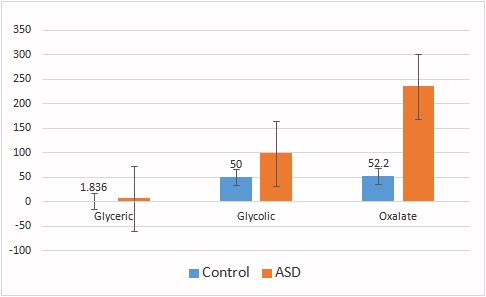 |
Glycolysis metabolites that cannot be used for energy can be converted to glycerate, glycolate and oxalate, all of which are elevated in children with ASD, supporting the concept of a block at pyruvate dehydrogenase. The accumulation and secretion of lactate, pyruvate, glycerate, glycolate and oxalate represent a significant loss of energy to the brains of kids with ASD. Poor metabolism of glucose is commonly associated with the development of diabetes. The incidence of diabetes in pregnant mothers is increasing (4,5,6), and has been shown to be associated with an increased risk of having a child with autism. It has also been associated with low vitamin B12 levels during pregnancy (4,5,6,7), a problem that is often not addressed during pregnancy (4,5). Gestational diabetes is also associated with lower birth weight babies, common in babies that later show signs of Autism.
Summary: ASD individuals have a metabolic block in the enzyme pyruvate dehydrogenase.
Metabolism of Fatty Acids in Autism
The preferred energy source for the heart is fat, but in sugar deficiency the body can try to make glucose from the small glycerol moiety that joins the fatty acids together. The released free fatty acids should be accessible for energy production provided the body has enough of the active form of vitamin B2, called FAD.
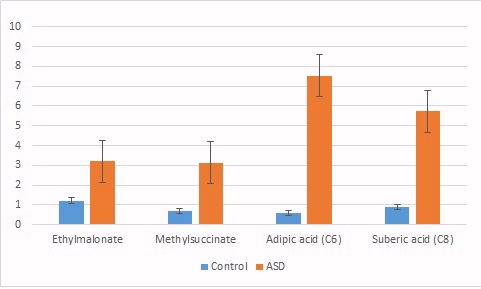
Examination of the fatty acid metabolites, ethylmalonate, methylsuccinate, adipic acid, and suberic acid, excreted into urine, shows them all being elevated in ASD. Once again, this represents a significant energy loss to the child and points to an inability to break-down these metabolites into acetyl-CoA for introduction into the Krebs cycle, or for the production of acetylcholine. The elevation in these fatty acids is typically associated with functional vitamin B2 deficiency.
Poor metabolism of fat is associated with obesity, and obesity in mothers is a risk factor for autism in the young and is also associated with vitamin B12 deficiency in the mothers (7,8)
Summary: ASD individuals have a metabolic block in the use of fat as an energy source.
Energy Production in Krebs Cycle in Autistic Individuals
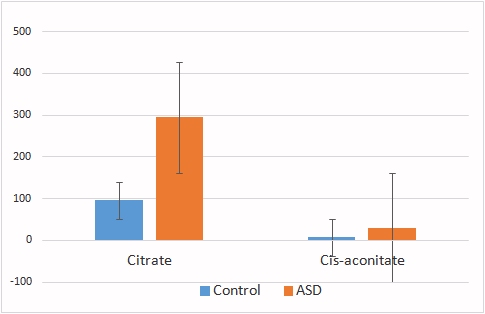
The metabolic break-down products of sugars, fats and proteins, are converted to energy by a series of enzymatic reactions in the Krebs cycle, which ultimately transfers energy to the electron transport chain to generate the universal energy unit, ATP. The efficiency of conversion is dependent upon the rate of these enzymatic reactions, and in conditions where the enzymatic reactions are constricted or slowed there is an elevation of the metabolic by-products in urine.
Comparison of the Krebs cycle intermediates from normal individual (control) and ASD individuals reveals significant blocks in the enzymes aconitase (which metabolizes citrate), alpha-ketoglutarate dehydrogenase, and succinate dehydrogenase, resulting in increased levels of the by-products citrate, cis-aconitic acid, alpha-ketoglutarate, and succinate. These blocks result in massive energy loss in the children and would dramatically reduce neuronal activity and brain function.
|
|
|
|
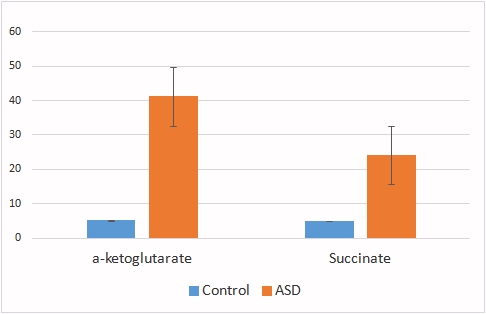
Summary: ASD individuals have a number of metabolic blocks in Krebs cycle.
Vitamin Status in Autism
Vitamin B12 deficiency is common in Autism
It has been known for some time that the level of vitamin B12 in the brains of autistic children is much lower than in normal individuals (7). Vitamin B12 is only used by two enzymes in the body, methylmalonyl-CoA mutase (adenosyl B12) and methionine synthase (methyl B12). Adenosyl B12 serves as a co-factor for the processing of several amino acids for energy, and lack of activity of the enzyme leads to build up of the metabolic by-product methylmalonic acid (MMA). Elevated levels of MMA can lead to the incorporation of abnormal lipids in the insulating layer (myelin sheath) of nerves. Methyl B12 serves an essential role in the methylation cycle, and in processing some forms of dietary folate.
|
|
|
|
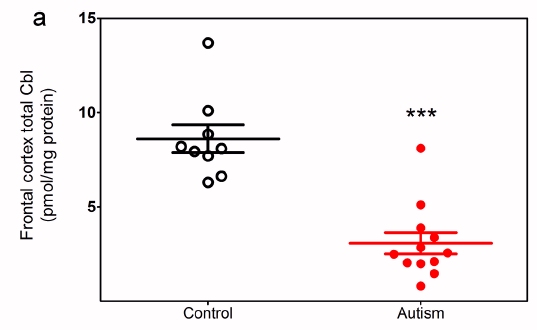
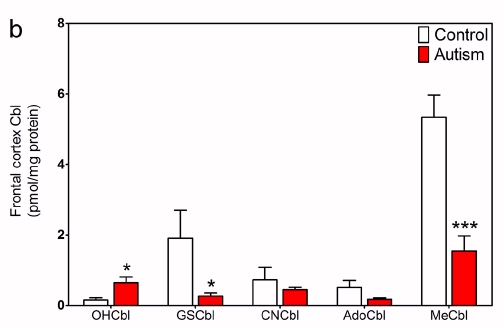
Data from Zhang etal, (15)
As can be seen from Zhang's work, the total amount of B12 is significantly lower in the brains of ASD kids, with the amount of methyl B12 and Adenosyl B12, lower than 30% of that of normal individuals. A deficiency of methyl B12 has been associated with lack of methylation in over 200 reactions in the body, including methylation of myelin basic protein, an essential component of lipid membranes. It is also involved in the final step in the production of melatonin and adrenalin. The lack of methyl B12 has major implications in normal development, and melatonin has also been implicated in neuronal maturation (16), the development of memory (17,18) and with the induction of sleep following feeding. Peripherally, melatonin has also been implicated in the maturation of the intestinal lining and stimulation of lactase, the enzyme that cleaves lactose in milk(19). Further, it is known that vitamin B12 deficiency alone can causes developmental delay (20-24) and poor neurodevelopment and lack of cognitive functioning (25). Vitamin B12 is crucial for differentiation of neuronal stem cells and for myelination of the central nervous system (26) B12 deficiency has also been associated with stunting in children, and the maternal vitamin B12 status is related to the height of the child several years later (27-28).
Levels of MMA have been found to be elevated in the urine of autistic individuals, indicating a deficiency in vitamin B12. Such deficiency results in decreased energy production, due to lack of activity of MMA-CoA mutase, and also due to lack of activity of aconitase (see above). It also would result in poor development of the villous tips (runting) in the intestine of these kids leading to reduced maturation of the gut, poor nutrient absorption, and reduced activity of lactase, leading to potential milk intolerance, particularly after weaning.
|
|
Significantly elevated MMA levels, indicative of B12 deficiency were found in the urine of all ASD kids tested. The urinary Organic Acids Test Data supports the findings of Zhang and co-workers (15), and suggests that either the lack of B12 is absolute (as per Zhang), or is due to functional deficiency, possibly due to absence of vitamin B2 or folate. Data from ASD children ranging in age from 1 to 18 years. Summary of 160 children.
It is known that the majority of vitamin B12 loading of the brain occurs during foetal development where as much as 17% of transplacentally derived vitamin B12 enters the foetal brain. Loading continues until the time of birth and thereafter very, very little enters the brain (30,31). As such foetal loading of the brain is incredibly important for the developing child, and deficiency of vitamin B12 in the mothers has a profound effect on the foetus and new-born child. Deficiency of vitamin B12 in the mothers is also correlated with deficiency of vitamin B12 in the neonate. An alarming rate of vitamin B12 deficiency in pregnant mothers in the UK has recently been reported (10,11,12), with more that 20% of women deficient as assessed by the haematological definition of deficiency (<150 pmol/L), but a whopping 70% being deficient if assessed by metabolic parameters (<250 pmol/L; 10,11,12). It would appear that the rates may have been dropping for some time, because in 1968 (before UK joined the EU), the average B12 levels were much higher at 288 pmmol/L (12) The rates of deficiency were much higher in India, where 43% were deficient (<150 pmol/L; 18). Hopefully this is not a portend of ever increasing rates of autism. Additionally, despite the diagnosis of B12 deficiency, the mothers in the various studies were not treated for B12 deficiency! The incidence of B12 deficiency in pregnancy seems to be very high, with over 50% of woman in Canada being metabolically deficient in the first trimester (30)
Vitamin B12 is known to be crucial for the development of myelination of the central nervous system, and poor vitamin B12 status is lined to poor growth and neurodevelopment (31), and neural tube defects (26). Thus, vitamin B12 deficiency in the mothers, which is later seen in the children, would be expected to have adverse outcomes. Further, maternal vitamin B12 status early in gestation (28 weeks) has been positively associated with child's subsequent mental and social development quotients, as measured at 2 years (26). This would "fit" with the critical time for foetal brain loading of the child (30,31). Furthermore, vitamin B12 deficiency, particularly of methyl B12, results in lower production of the methylating agent, S-Adenosylmethionine (SAM). Lower SAM in turn leads to lower energy production of creatine (the essential backbone for creatine-phosphate) and ubiquinol (CoQ10), the essential electron transfer molecule in the Electron Transport Chain. Low CoQ levels have been associated with lower cognitive function and intellectual disability in autism (21). Reduced production of SAM also affects the activity of the histamine-neutralizing enzyme, Histamine-N-methyl transferase, and would explain much of the food insensitivity of young children with ASD, due to the presence of histamine in a diverse range of foods.
The typical symptoms of vitamin B12 deficiency in the neonate are very similar to those observed in autism and include megaloblastic anemia, feeding difficulties, developmental delay, microcephaly, failure to thrive, hypotonia, and cerebral atrophy with symptoms of lethargy, and occasionally seizures (95), and psycho-motor delay. Vitamin B12 deficiency is associated with reduced object recognition and problems with both short and long-term memory (101).
Vitamin B12 Deficiency in Vegetarian Mothers
Children born of vegan and vegetarian mothers often have moderate to severe vitamin B12 deficiency (29-52), and such deficiencies have been associated with delayed myelination, weight loss, and reduction of motor skills, delayed development, neuroregression, regression of psychomotor development, growth retardation, brain atrophy and apathy. Despite these deficiencies being well documented, for more than 30 years, many vegetarian and vegan mothers do not supplement before, during or after pregnancy, nor do their health professionals check them for deficiency.
Maternal serum B12 levels are closely correlated with the vitamin B12 levels in the mother's milk

Vitamin B12 deficiency in the milk has been found to be measurable by an increase in MMA levels in the urine of the mothers, and B12 levels in the mothers are mirrored in MMA levels in the infants (reprod from Specker et al, 1990(61)) .


As one would expect increased urinary MMA in babies was inversely correlated with serum vitamin B12 levels in the infants (reprod from Specker et al, 1994(61)).

Summary: Babies born to vitamin B12 deficient mothers are vitamin B12 deficient. ASD individuals are deficient in functional Vitamin B12
Vitamin B2 deficiency in Autism
Vitamin B2 (riboflavin), is technically a pro-vitamin or vitamin precursor, which when activated is involved in over 100 different metabolic reactions within the body. Vitamin B2 activation is primarily under the control of the thyroid gland where the thyroid hormone (T4) is initially made. The formation of T4 or tetraiodothyronine (thyroxine) requires the presence of sufficient iodine in the diet, and in dietary insufficiency the levels of T4 are low. T4, however, is a pro-hormone and must be converted to T3 (triiodothyronine) by the selenium dependent iodothyronine deiodinase. The fetus produces T4 at about 18-20 weeks of gestation, but does not make T3 until 30 weeks of gestation. This is dependent, however, on the mother receiving sufficient Iodine (150-300 ug/day) and Selenium (55-200 ug/day) so that the fetus can make T4 and T3. T3 has many functions in the body, but one important function is to turn on the production of the enzyme riboflavin kinase, which converts dietary riboflavin to riboflavin mononucleotide (FMN). Finally, FMN is converted to Flavin-adenine dinucleotide (FAD) by the Molybdenum dependent enzyme FAD synthase. In data that has generously been supplied to us by mothers of autistic children, over 50% were deficient in Iodine, over 80% were deficient in Selenium and around 50% were deficient in Molybdenum. Either or combined deficiency in Iodine, Selenium or Molybdenum, would lead to lack of conversion of dietary or supplemental riboflavin to the active forms FMN and FAD.
|
|
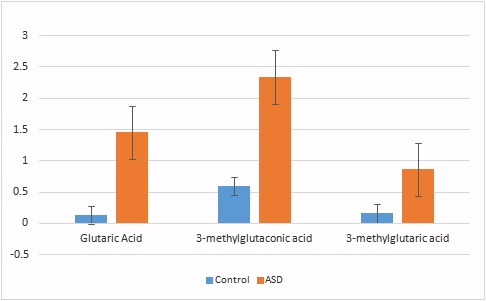
Metabolically lack of FAD can be measured by a reduced ability to burn fat, with an increase in ethylmalonate, methylsuccinate, adipic acid, and suberic acid (see above), and by an increase in glutaric acid, and by reduced function of pyruvate dehydrogenase (with increased pyruvate and lactate - see above). Interestingly, accompanying the increase in glutaric acid there is also an increase in the metabolites, 3-methlglutaconic acid, and 3-methylglutaric acid, both of which are break-down products of leucine, but suggest that FAD is used by the enzyme 3-methylglutaconyl-CoA hydratase. Each of these markers is significantly increased in the urine of autistic children, demonstrating a functional deficiency in vitamin B2. Often this deficiency is further increase when children are deliberately removed from one of their major sources of dietary B2, namely dairy, and particularly dairy milk. Increased urinary excretion of 3-methygluaconic and 3-methylglutaric acid has been associated with developmental language delay (22).
Summary: ASD individuals are deficient in functional Vitamin B2
Autophagia in Autism. In severe functional vitamin B2 deficiency, the autistic child is progressively less able to obtain energy from fats or sugars, and so must resort to obtaining energy from protein breakdown. In children on a limited protein diet, such as children from a vegetarian or vegan family, supply of protein from the diet may be very limited, and the child then starts a process of self-cannabalism, or autophagia. In this process the child starts to break-down its own muscle tissue for energy, with the result that the child becomes gradually thinner and thinner and has very poor muscle tone. A feature of this condition is the production of very high levels of oxalates in urine, with levels reaching forty times that seen in metabolically normal individuals. Similar autophagia is seen in the terminal stages of Alzheimer's Disease. Oxalate production in these individuals comes from the breakdown of high glycine and hydroxyproline containing "Self-collagen", rather than from eating very, very high content oxalate foods.


Vitamin B1 and biotin deficiency in Autism. Many of the autistic children also show signs of vitamin B1 and biotin deficiency, it is not however possible to assign this a causative role in the development of ASD, as nutritional lack is often "imposed" upon the children when they are taken off a standard diet and placed on the nutritionally poor gluten free and casein free diets. This then can cause additional vitamin B1 deficiency, extended vitamin B2 deficiency, calcium deficiency, selenium deficiency, iodine deficiency and molybdenum deficiency. Further the diet does not reverse the developmental delay and as such we are definitely not in favour of these nutrient selective/restrictive diets. The nutritional intake can be further restricted if the child is taken off eggs, hence creating a biotin deficiency to add to the poor child's woes.
Iron deficiency in Autism
For many years, it was thought that iron was solely involved as part of the structure of the heme molecule such as in the structure in hemoglobin. More recently it has been recognized as an important factor in the activity of iron sulphur proteins, such as aconitase, succinate dehydrogenase, and more recently gamma-aminobutyrate amino transferase (GABA-AT) and lipoate synthase. Brain accumulation of iron appears to happen primarily in utero, and uptake of iron into the brain, posting weaning, is limited (63). Iron is critical for myelination of nerve cells, and lack of myelination causes slower neuronal conduction, abnormal reflexes in children, and deficits in auditory and visual function (62). Iron deficiency has also been associated with poorer language and global IQ, and social and attention problems. Iron-deficiency anemia is an advanced stage of iron deficiency, however, early Iron deficiency is associated with cognitive alterations in adolescents, and with developmental delay in children. Iron deficiency is generally associated with reduced levels of the iron storage protein, ferritin and ferritin levels are significantly lower in ASD kids (28.6 ug/L +/- 22 ug/L) when compared to normal individuals (152 ug/L +/- 142 ug/L). Deficiency of activity of Fe-S proteins has been shown to result in lower energy output in Krebs cycle and the electron transport chain, and also lack of emotional control due to lack of activity of GABA-AT, with increased anxiety. Increased levels of GABA are characteristic of iron deficiency (54). Iron has a critical role in the formation of the myelin sheath around neurons, and iron deficiency in mothers has shown a higher incidence of conditions such as ASD, and has also been associated with irreversible alterations in myelin (65). Iron deficiency in the brain precedes the signs of iron deficiency in RBC production. Serum ferritin levels below 76 ug/L are associated with abnormalities in neonatal recognition memory, and neuronal processing (66-71). Further, a recent study has shown that lower iron levels (as judged by serum ferritin) are associated with decreased brain activity and lower energy expenditure, as well as a reduced heart rate (31). Iron is known to be critical in neurodevelopment, and fetal iron deficiency has been shown to result in acute brain dysfunction, with long-lasting abnormalities even after repletion (72-77). Lower iron is also associated with restless leg syndrome and febrile seizures, which are common in children with ASD (78-82). Seizure rates were increased in children on soy infant formula, presumably due to the lower iron content (81). Iron deficiency is associated with a greater risk of headache, particularly if blood pressure is elevated. Worryingly, iron deficiency is still be defined by clinicians in term of iron deficiency anemia, and values of 12 or 15 ug/L ferritin being commonly used to assign deficiency (84). Thus, children who have many of the signs assigned to iron deficiency, such as reduced cognition, developmental delay, depression, poor neuronal processing, anxiety, migraine headaches, restless leg syndrome and febrile seizures, are not being treated for iron deficiency due to clinicians sticking to archaic, anemia defined, definitions of iron sufficiency. Our studies have shown reduced energy production by aconitase and succinate dehydrogenase when serum ferritin levels drop below 70 ug/L (85-88).
Summary: Iron deficiency is common in ASD individuals and can be associated with lower energy production in Krebs cycle, reduced myelination, delayed mental development and febrile seizures.
Vitamin D deficiency is common in Autism
Paralleling the rapid rise in the incidence of ASD in many countries has been the adoption of high SPF value cosmetics in many countries. Thus, when compared to the early 1990s, where very few "daily" cosmetics had any SPF protection in them, in 2018 many "daily" cosmetics "boast" SPF values of 60+ and above. Vitamin D has a critical role in brain development, and even transient deficiency in the womb can result in delayed brain development (89). Further studies comparing vitamin D sufficient and vitamin D deficient children showed more autism related traits in those who were born to mothers with vitamin 25-OH-D concentrations less than 25nmol/L (90). Similarly, lower vitamin D levels in the first trimester of pregnancy have also been associated with a higher risk of autism (52). It has also been shown that lower vitamin D levels are common in ASD children than in age matched controls (91-93). Associated with this has been a massive increase in the rate of vitamin D deficiency. Thus, in the period 2000 to 2014 there was a fifteen-fold increase in the rate of vitamin D deficiency in children in the UK (96).
Neurotransmitter metabolites in Autism
|
|

Many theories on the development of autism have postulated that there is some sort of alteration in the mental function of these children. Such theories have suggested an alteration in the functional organization in the brains of these individuals, some odd "gut dysbiosis" which affects the brain, or many other unproven associations between vaccines, mercury and other factors. It is though possible to gain some insight as to what may be happening in the brains through the analysis of urinary organic acid, which can also be used to monitor alterations in the break-down products of the neurotransmitters dopamine, nor-epinephrine, epinephrine (adrenalin), serotonin and melatonin.
|
|
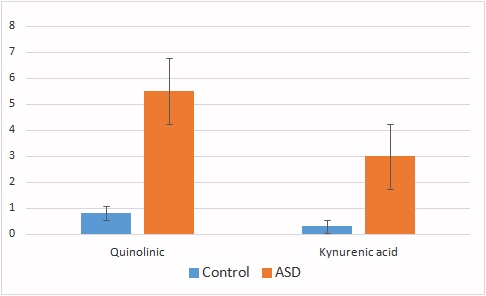
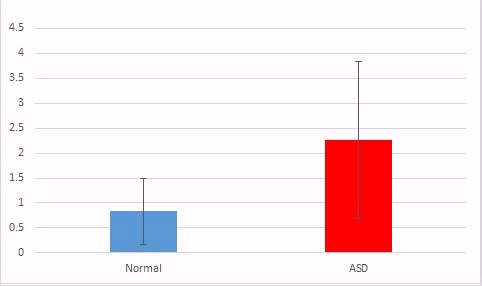
Examination of the urine of ASD children revealed massively increased levels of the neurotransmitter break-down products QA, KA (shown) and VMA/HVA (not shown). Such elevations have been associated with conditions such as Alzheimer's disease and also schizophrenia. The metabolites themselves are also known to be quite neurotoxic. The levels of elevation were directly related to MMA and glutaric acid levels, reflecting a possible causality of low vitamin B12 and/or low vitamin B2.
Summary: ASD individuals have altered neurotransmitter metabolites, which show similarities to people with dementia.
Behaviour and ASD
Serotonin in the brain has been shown to regulate anxiety, and aggressive behavior, via the 5HT1A receptor (a specific serotonin receptor) as well as having activity in coping, cognitive flexibility, and creative thinking, via the 5HT2A receptor (a second type of serotonin receptor). Many children with ASD have greatly enhanced anxiety, show aggressive behaivour and are unable to cope, have limited cognitive flexibility. Initially this was thought to be due to lack of production of serotonin, however many studies have shown an over-production of serotonin in the brain of children with ASD. Individuals with vitamin B12 deficiency have also been shown to have issues with anxiety, aggressive behaviour, an inability to cope, or are unable to "think outside the box" or have reduced creativity. These individuals have also been shown to over-produce serotonin, however, in ASD serotonin production can reach levels 50-200 times normal. Such extreme levels of serotonin would effectively down-regulate the 5HT1A and 5HT2A receptors, and hence lead to symptoms typically ascribed to serotonin deficiency.
Summary: Extreme vitamin B12 deficiency in ASD individuals results in over-production of serotonin, down regulation of serotonin receptors, and can result in behavioural characteristics typical in these children.
Bioenergetic Deficiencies in ASD
A study of the urinary metabolites from ASD children of ages 1 to 18 years showed a uniform deficiency in both vitamin B2 and vitamin B12. These deficiencies, when combined with the lower levels of iron in these individuals strongly suggest that deficiency of B2/B12 and iron in the womb has lead to the delayed development seen in these children. This delay manifests itself in reduced and inefficient energy production in mitochondria, altered neurotransmitter metabolites, and resultant developmental delay. Fetal Insufficiency of iron or vitamin B12 alone has been correlated with lower cognitive function and poor development in neonates (27, 14). Clearly, adequate dietary intake of iron, vitamin B2 and vitamin B12 before, during and after pregnancy is critical for the child's development and women who fail to do this potentially have a highly elevated risk of giving birth to a child who will subsequently show the developmental delay(s) that are characteristic of ASD. The biochemical abnormalities would contribute to the known mitochondrial dysfunction that is typical of many mitochondrial diseases (58-63). Other known mitochondrial diseases include cerebral palsy, Parkinson's disease, epilepsy, Alzheimer's disease, Huntington's disease, developmental delay, Chronic Fatigue, Fibromyalgia, Lou Gehrig's, Atypical Learning disorder, muscular dystrophy.
Summary: ASD individuals have typical bioenergetics to that seen in Mitochondrial diseases.
Nutritional Risks for the Development of Autism
Clearly the biochemical deficiencies that are associated with ASD most likely occur in the womb of mothers, hence all mothers should ensure that before they think of conceiving they reduce the nutritional risks, which can generally be done with a standard multivitamin preparation, however, since deficiencies in Iodine, Selenium and Molybdenum are common in ASD children, mothers must supplement with these or ensure adequate dietary intake. Whilst it is generally suggested that women supplement with folate, before and during pregnancy, the suggestion to supplement with other vitamins and iron, clearly would be desirable.
Iron: Recommendations to pregnant women is that ferritin should be above 70 ug/L, BUT, evidence of iron deficiency can already be seen at this level, and hence a value of 100 would seem a more logical minimum. Energy levels start to reduce at ferritin levels below 70 ug/L.
Vitamin B12: Measurement of serum B12 is very controversial, particularly in the early stages of B12 deficiency. Vitamin B12 levels drop progressively during pregnancy, and a drop in serum vitamin B12 of greater than 50 pmol/L is very common. Vitamin B12 levels in mothers parallel that in the child. Since vitamin B12 deficiency, as measured by elevated homocysteine and methylmalonic acid (MMA), starts to occur at levels below 250 pmol/L, logically mothers should be above 300 pmol/L before entering pregnancy, and levels of MMA and Homocysteine should be low. The risk of neural tube defects increases as levels drop below 300 pmol/L in the mothers.
Vitamin B2 (riboflavin): Measurement of functional vitamin B2 is extremely uncommon in general practice, however, riboflavin, just like iron and B12 drops during pregnancy. Riboflavin deficiency should be suspected if a mother is over-weight, has diabetes, high blood pressure, or experiences gestational diabetes, carpal tunnel syndrome, or is on a diet known to be deficient in riboflavin, such as a diet low in dairy. Such a diet is highly contra-indicated due to the potential co-deficiency in iodine and more particularly calcium. Similarly a diet low in Iodine, Selenium and/or Molybdenum would result in functional B2 deficiency. In this regard diets high in Soy or Gluten-free diets are particularly prone to Iodine/Selenium and Molybdenum deficiency. Prolonged functional vitamin B2 deficiency, eventually leads to the production of functionally inactive vitamin B12, both of which are typical in autistic children.
Iodine: Iodine deficiency is the single most common cause of preventable mental impairment worldwide, and affects around 2 billion people worldwide. Governments around the world and WHO have recognized this and have instituted programmes to reduce Iodine deficiency through mandatory Iodination of salt, supplementation of cows with Iodine to produce milk with Iodine in it, and in some countries they have mandated the use of Iodine in bread. Not all countries, however, have adopted these recommendations, and in Israel, which has not adopted mandatory fortification of salt, over 80% of pregnant women have been shown to have inadequate daily intake of Iodine. Despite mandatory fortification of salt in the US, and despite the known need for adequate Iodine during pregnancy, over 50% of women admitted to maternity wards in Boston (USA) were found to have to insufficient Iodine uptake. Further, since 1970 average Iodine intake in the US has decreased by 50%. In India, there are around 500 million people who are Iodine deficient, 54 million with goiter and 2 million with cretinism. Adoption of milk alternatives (soy, almond "milk" etc), low dairy intake and chose of "gluten-free" diets, and adoption of alternative salts such as Iodine free sea salt, Himalayan rock salt and non-iodized salt, are possible reasons for the deficiency. Further despite many governments now mandating Iodine-fortification of bread, many companies supplying Bread-mixes to not fortify the mix. Persons at risk include vegans, individuals with real or perceived lactose intolerance, or those with minimal dairy intake. Studies on school children in the UK found that over 50% of 14-15 year old girls were receiving insufficient Iodine in their diet (55). Something that would seem inconceivable given the amount of information on the importance of Iodine that is in the literature and in the dietary advice for pregnant women. In this regard, over 50% of children with autism were found to be Iodine deficient. Due to their importance in the activation of vitamin B2, deficiency of Iodine, Selenium, and/or Molybdenum would effectively have a very similar consequence. Our studies have shown that over 80% of children with autism were selenium deficient and 50% Molybdenum deficient.
Selenium: Selenium deficiency is very common in children with autism and over 80% of individuals with autism have been found to be deficient by hair metals analysis. Dietary intake of Selenium is now less than the RDA in the United Kingdom, and has been known to be low in New Zealand for over 20 years, due to low Selenium levels in the soil. Persons on gluten-free diets, or on diet low in dairy products are at risk of Selenium deficiency. Selenium deficiency in the soil has been associated with mental retardation, spastic diplegia, and spastic gait with a disturbance of gait. it has been estimated that as many as 1 billion people world-wide are Selenium deficiency, a deficiency that is increasing. The RDA for selenium is not achieved in the majority of European countries, UK, parts of China, parts of Africa, Asia, and New Zealand (97).
Molybdenum: Molybdenum deficiency is very common in children with autism and over 50% of individuals with autism have been found to be deficient by hair metals analysis. Molybdenum deficiency is quite regional throughout the world, with many states in the USA having low levels of Molybdenum in the soils. Curiously the rates of obesity in the US are inversely proportional to the levels of Molybdenum in the soil. Molybdenum deficiency can result in an inability to properly process sulphites, and has been associated with the development of epilepsy and seizures (Sharma and Prasad, 2017; Slot etal, 1993). Molybdenum deficiency has also been associated with reduced production of expressive language (Scelsa etal, 2019)
Vitamin D: Vitamin D is essential for neuronal development. The advent of high SPF value cosmetics and the increase in hours worked indoors has seen a rise in the incidence of vitamin D deficiency. Further, the reduction in the consumption of dairy products and the switch to alternative products such as soy, and almond drinks, and adoption of a vegan diet. Current recommendations are a daily intake of at least 600 IU per day, however many studies suggest that a minimum of 1000 IU per day, particularly during pregnancy. Vitamin D deficiency has been defined as less than 50 nmol/L (20 ng/ml). Vitamin D deficiency is very common in some countries, and over 42% of Singapore residents (92), 45.5% of Saudi residents, and in 2018 over 82.5% of females in South Korea (an increase from 76% in 2008)(93) were found to be vitamin D deficient. Vitamin D status decreases with increases in weight (one of the predisposing maternal factors for giving birth to a child with ASD). There has been a massive increase in the rate of vitamin D deficiency in the US with a 15-fold increase between 2000 to 2014 paralleling the massive increase in the rate of autism seen in the US over that time (94). In Australia in 2012, 30% of women of child bearing age were found to be vitamin D deficient.
"Nexus Theory™": The combined deficiencies of Iron/B12/B2 and Vitamin D come together as a Nexus, which appears to be the crux of the development of autism and forms the basis of the "Nexus Theory™" of Autism. The theory is explained at NexusTheory
Treatment of Autism
Clearly any treatment for autism must overcome the nutritional deficiencies before progress can be made in fixing the developmental delays associated with autism and also with the delayed myelination found in autism. Given that deficiencies in any of iron, vitamin D, vitamin B12, and biotin all are causative for delayed myelination, and all are associative for the development of dementia, one can logically argue that if these deficiencies are not fixed, then the person with autism cannot reverse the condition.
Early Warning Signs of Potential Problems
In the best case scenario, a woman will prepare herself for her pregnancy by checking her nutritional status before she becomes pregnant, however, if this has not been the case there are many potential warning signs of nutritional deficiency
-
Difficulty in becoming pregnant
-
Frequent miscarriages
-
Gestational Diabetes
-
Premature or Pre-term delivery - low gestational age
-
Previous child with Autism
-
Maternal obesity
-
Maternal hypothyroidism
-
Depression during pregnancy and use of antidepressants
-
Fatigue during pregnancy
-
Low intake of iron during pregnancy
-
Restless Leg Syndrome
-
Vitamin D deficiency in the mother and child
-
Male child
-
Low ferritin levels during pregnancy - having to supplement during pregnancy
References/ Useful links.
-
Bougma etal, 2013 Iodine and mental development of children 5 years old and under... 3794354
-
Kapil 2007 Health Consequences of Iodine Deficiency 3074887
-
Gastadi etal 2014 Iodine deficiency and its consequences for cognitive and psychomotor development of children 4132543
-
Saloojee 2001 Iron deficiency and impaired child development 1121846
-
Sidrak etal 2014 Iron deficiency in children with global developmental delay and autism spectrum disorder 24372984
-
Lozoff 2007 Iron deficiency and child development 1564826507284S409
-
Black 2011 Effects of vitamin B12 and folate deficiency on brain development in children PMC3137939
-
Jain etal 2015 Vitamin B12 deficiency in children: a treatable cause of developmental delay 24453156
-
Rasmussen etal, 2001 Vitamin B12 deficiency in children and adolescents S0022
-
Sukumar etal, 2016 Vitamin B12 status among pregnant women in the UK and its association with obesity and gestational diabetes. PMID 27916927
-
Knight etal 2015 Lower circulating B12 is associated with higher obesity and insulin resistance during pregnancy in a non-diabetic white British Population. PMID
-
Low-Beer, etal, 1968 Serum vitamin B12 levels and vitamin B12 binding capacity in pregnant and non-pregnant Europeans and West Indians PMID 5681054
-
Krishnaveni etal, 2009 Low plasma vitamin B12 in pregnancy is associated with gestational 'diabeity' and later diabetes. PMID 19707742
-
Lai etal, 2017 High folate and low vitamin B12 status during pregnancy is associated with gestational diabetes PMID: 28381340
-
Zhang etal, 2016 Decreased levels of vitamin B12 in aging, autism and schizophrenia. PMID: 26799654
-
Chu etal, 2016 Effects of melatonin and its analogues on neural stem cells. PMID 26499359
-
Rudnitskaya etal, 2015 Melatonin Attenuates Memory Impairment, Amyloid-β Accumulation, and Neurodegeneration in a Rat Model of Sporadic Alzheimer's Disease. PMID 26402759
-
Shen etal, 2016 Effect of Melatonin and Resveratrol against Memory Impairment and Hippocampal Damage in a Rat Model of Vascular Dementia. PMID 28419991
-
Li etal, 2017 Effect of Melatonin on renewal of chick small intestinal mucosa PMID 28431176
-
Whiton etal, 1979 Brain damage in infancy and dietary B12 deficiency PMID 502936
-
Smolka etal, 2001 Metabolic complications and neurological manifestations of vitamin B12 deficiency in children of vegetarian mothers. PMID 11787236
-
Zengin etal, 2008 Clinical manifestations of infants with nutritional vitamin B deficiency due to maternal dietary deficiency PMID 18945280
-
Halicioglu etal, 2011 Nutritional deficiency in infants of vitamin B12 deficient mothers PMID 99429203
-
Demir etal, 2013 Clinical and neurological findings of severe vitamin B12 deficiency... PMID 23781950
-
Kvestad etal Vitamin B12 status in infancy is positively associated with development and cognitive functioning 5 y later in Nepalese children. Am. J. Clin Nut. 2017 105(5):1122-1131
-
Strand etal, The effect of vitamin B12 supplementation in Nepalese infants...Trials, 2017: 187
-
Strand etal, Maternal and infant vitamin B12 status during infancy predict linear growth at 5 yrs, Ped Res 2018 https://doi.org/10.1038/s41390-018-0072-2
-
Smith, AD 2018 Maternal and infant vitamin B12 status and development. Ped Res. https://doi.org/10.1038/s41390-018-0110-0
-
Guez etal, 2012 Severe vitamin B12 deficiency in an exclusively breastfed 5-month-old Italian infant born to a mother receiving multivitamin supplementation during pregnancy PMC 22726312
-
Roed etal, 2008 Severe vitamin B12 deficiency in infants breastfed by vegans (Ugesr Laeger, 171: 3099-101
-
Agrawal and Nathani, 2009 Neruo-regression in vitamin B12 deficiency MBJ 2009
-
Chalouhi et al, 2008 Neurological consequences of vitamin B12 deficiency and its treatment. Ped Emerg Care, 24: 538-41
-
Lucke et al, 2007 Maternal vitamin B12 deficiency: cause for neurological symptoms in infancy. Z Geburtshilfe Neonatol, 211: 157-161
-
Strucinska 2002 Vegetarian diets of breastfeeding women in the light of dietary recommendations. Rocz Panstw Zakl Hig 53: 65-79
-
Rendle-Short et al 1979 Vegan mothers with vitamin B12 deficiency. Med J Aust 3:483
-
Michaud et al, 1992 Nutritional vitamin B12 deficiency: two cases detected by routine newborn urinary screening. Eur J Pediatr. 151;218-20
-
Specker 1994 Nutritional concerns of lactating women consuming vegetarian diets. Am J Clin Nutr. 59: 1182S
-
Renault et al 1999 Neuropathy in two cobalamin-deficient breast-fed infants of vegetarian mother. Muscle Nerv 22:252-4
-
Ueland and Monsen 2003 Hyperhomocysteinemia and B-vitamin deficiences in infants and children. Clin Chem Lab Med. 41:1418-26
-
Weiss et al, 2004 Severe vitamin B12 deficiency in an infant associated with maternal deficiency and a strict vegetarian diet. J Ped Hem Oncol. 26:270-1
-
Jarosz et al, 2004 Vitamin B12 deficiency anaemia in a 7.5 months old girl. Med Wieku Rozwoj 8:283-8
-
Baatenburg et al 2006 Developmental delay in breastfed children due to inadequate diet of the mother. Ned Tijdshr Geneeskd 150: 465-9
-
Kollee 2006 Vitamin deficiencies in breastfed children due to maternal dietary deficiency. Ned Tijdschr Geneeskd. 150:473-6
-
Yajnik 2006 Nutritional control of fetal growth. Nutr Rev. 64: S50-1
-
Cetinkaya etal, 2007 Nutritional vitamin B12 deficiency in hospitalized young children. Ped. Hem. Onco. 24:15-21
-
Fadyl and Inoue 2007 Combined B12 and iron deficiency in a child breast-fed by a vegetarian mother. J Ped Hemato Oncol. 29:74
-
Mathey et al, 2007 Failure to thrive and psychomotor regression revealing vitamin B12 deficiency in 3 infants. Arch Ped 14: 467-71
-
Dror and Allen, 2008 Effect of vitamin B12 deficiency on neurodevelopment in infants... Nutr Rev. 66:250-5
-
Honzik et al, 2010 Clinical presentation and metabolic consequences in 40 breastfed infants... Eur J Paed Neurol. 14:488-95
-
Kocaoglu et al, 2014 Cerebral atrophy in a vitamin B12-deficient infant of a vegetarian mother. J Health Pop Nutr 32:367-71
-
Bravo et al, 2014 Hematological and neurological compromise due to vitamin B12 deficient in infant of a vegetarian mother... Rev Chil Ped 85:337-43
-
Bousselamati et al. 2018 Psychomotor regression due to vitamin B12 deficiency. Pan Afr MEd J 20:30
-
Hare etal, 2013 A delicate balance: Iron metabolism and diseases of the brain... PMIC 3715022
-
Guevara-Campos etal, 2015 Autism and intellectual disability associated with mitochondrial disease and hyperlactacidemia.. PMID 25679448
-
Bravo etal, 2014 Haematological and neurological compromise due to vitamin B12 deficient in infant of a vegetarian mother.... PMID 25697251
-
Schroder etal 2017 Pregnant women of South Asian Ethnicity in Canada have substantially lower vitamin B12 status compared with pregnant woemen of European ethnicity PMID 28920568
-
Chandyo etal, 2017 The effects of vitamin B12 supplementation during pregnancy PMID 28851784
-
Woods etal, 1960 Vitamin B12Co-60 readily passes the placenta into fetal organs and nursing provides B12 from mother to pup... PMC 2137236
-
Graber etal, 1971 Placental transport of vitamin B12 in the pregnant rat PMID 5552402
-
Michelson etal, 1999 Urinary organic acid screening in children with developmental language delay PMID 10518282
-
Specker et al. 1990 Vitamin B12: Low milk concentrations are related to low serum concentrations in vegetarian women.....Am J Clin Nutr 52:1073-6
-
Specker et al. 1994 Vegetarian diets during lactation. Am J. Clin Nutr 59:1182S-6S
-
Kim and Wessling-Resnick, 2014 Iron and mechanisms of Emotional Behaviour PMID 618599
-
Geng etal, 2015 Impact of fetal-neonatal iron deficiency on recognition memory at 2 months of age PMID 618599
-
Armin etal 2010 In utero iron status and auditory nural maturation in premature infants as evaluated by auditory brainstem response PMID 19939407
-
Kwik-Uribe etal, 2000 Chronic marginal iron intakes during early development in mice result in persistent changes in dopamine metabolism and myelin composition.PMID 11053527
-
Choudhury etal 2015 Latent iron deficiency at birth influences auditory neural maturation in late preterm and term infants PMID 26310540
-
Armony-Sivan etal 2004 Iron status and neurobehavioral development of premature infants PMID 15318248
-
Wenger etal, 2017 Effect of iron deficiency on simultaneous measures of behavior, brain activity and energy.. PMID 28784049
-
Zumbrennen-Bullough etal 2014 Abnormal brain iron metabolism in Irp2 deficient mice is associated with mild neurological and behavioral impairments PMID 24896637
-
Georgieff 2008 The role of iron in neurodevelopment: fetal iron deficiency and the developing hippocampus PMID PMC2711433
-
Sherjil etal 2010 Iron deficiency anaemia - a risk factor for febrile seizures in children PMID 22338422
-
Fallah etal 2014 Iron deficiency and iron deficiency anemia in children with first attack of seizure and on healthy control group.... PMC PMC4135276
-
Gillberg etal 2017 Febrile seizures and epilepsy: Association with autism and other neurodevelopmental disorders in the child....... PMID 28754226
-
McCue etal 2016 Prevalence of non-febrile seizures in children with idiopathic autism spectrum disorder and their unaffected siblings....... PMID 27894273
-
Hara 2007 Autism and epilepsy: a retrospective follow-up study PMID 17321709
-
Westmark 2014 Soy infant formula and seizures in children with autism: a retrospective study PMID 24622158
-
Fallah etal 2016 Evaluation efficacy of ferrous sulfate therapy on headaches of 5-15 years old iron deficient children with migraine PMC
-
Ali etal 2016 Developmental vitamin D deficiency and autism: Putative pathogenic mechanisms. PMID 28027915
-
Vinkhuyzen etal 2018 Gestational vitamin D deficiency and autism-related traits PMID 27895322
-
Chen etal 2016 Lower maternal serum 25(OH) D in first trimester associated with higher autism risk in Chinese offspring PMID 27663117
-
Garipardic etal, 2017 Association of Attention Deficit Hyperactivity Disorder and Autism Spectrum Disorders with mean platelet volume and vitamin D PMID 28319054
-
Ariganjoye, 2017 Pediatric hypovitaminosis D: Molecular perspectives and clinical implications PMID 28229097
-
Endres etal, 2016 Vitamin D deficiency in adult patients with schizophreniform and autism spectrum disorders PMID 27766084
-
Vanderpump etal, 2017 Iodine status of UK schoolgirls: a cross-sectional survey PMID 21640375
-
Giulivi et al Mitochondrial dysfunction in autism. J. Am. Med Assoc 2010 304: 2387-2396
-
Chauhan etal Brain region-specific deficit in mitochondrial electron transport chain complexes in children with autism. J. Neurochem. 2011 117: 209-22
-
Tang et al Mitochondrial abnormalities in temporal lobe of autistic brain. Neurobiol Dis 2013 54: 349-361
-
Goh et al Mitochondrial dysfunction as a neurobiological subtype of Autism Spectrum Disorder.. JAMA psychiatry 2014 71: 665-671
-
Napoli et al Deficits in bioenergetics and impaired immune response in granulocytes from children with autism. Pediatrics 2014 133:e1405-10
-
Parikh et al A modern approach to the treatment of mitochondrial disease. Current Treatment Options in Neurology. 2009 11: 414-430
-
Bi et al. Prevalence of vitamin D deficiency in Singapore: Its implications to Cardiovascular Risk Factors. PMC4723156
-
Park et al. Vitamin D status in South Korean population... Medicine, 2018 97 Issue 26
-
Basatemur et al. Trends in the diagnosis of vitamin D deficiency. PMC5337117
-
Benbir et al. Seizures during treatment of vitamin B12 deficiency Seizure 2007 16: 69-72
-
Basatemur et al. Trends in the diagnosis of vitamin D deficiency Pediatrics 2017 139 PMC5337117
-
Huag; et al. How to use the world's scarce selenium resources efficiently... PMC2556185
-
Sharma and Prasad Inborn errors of metabolism and epilepsy:... IntJMolSci 2017, 18, 1384
-
Slot etal Molybdenum cofactor deficiency: am easily missed cause of neonatal convulsions Neuropediatrics 1993 24: 139-42
-
Scelsa etal Mild phenotype in Molybdenum cofactor deficiency: Mol Gen Gen Med 2018 7, e657
-
Jadavji etal Severe methylenetetrahydrofolate reductase deficiency ... Mol Gen Met 2012 106: 149-159
See also
www.autism-help.org/comorbid-mental-retardation.htm
https://worldneurologyonline.com/article/breakthrough-autism-prevention/
Copyright © 2014 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited